

The Vanderbilt. SPD. ABA.
The Vanderbilt. SPD. ABA.

Hello! Thanks for reading another issue of DBP in 1-2-3, a newsletter devoted to issues around child development and behavior from a medical perspective. While my goal is to provide clinically relevant information and guidance and keep personal commentary aside, I cannot go on without mentioning the issue of bringing children back to school in the COVID-19 era. It has become highly politicized with fear tactics to stifle progress and innovation. There is really no reason not to open schools for in-person learning if we follow the science (and there is quite a bit of it). We’ve reached an inflection point where the harm caused by keeping children at home for remote learning is greater than the harm from COVID-19. The AAP and other reputable child advocacy organizations are urging schools to reopen. On the front lines of my practice, I have heard anecdote after anecdote of suffering and regression from children learning remotely, especially those with special needs. There will be a windfall of research not too distant in the future confirming what many predict: negative ripple effects on academic achievement and emotional well-being in children and an even greater disparity between the haves and have-nots. There are disparities in how school districts deal with openings around the country, let alone the Bay Area. There is a clear precedent for opening up schools safely. It’s a sad state of affairs that some districts have not been able to find workable solutions because of incompetent leadership, political stonewalling by teacher unions, or simply being overwhelmed by inertia.
#1 Using the Vanderbilt for managing ADHD
ADHD is a clinical diagnosis. Contrary to popular belief, there are no definitive tests for ADHD. A good clinical history is the centerpiece of any ADHD evaluation. That being said, validated behavior rating scales or surveys do play a role. And yes, sometimes, psychological testing is warranted. This is especially true if there are concerns about a learning disorder or possible coexisting conditions like autism spectrum disorder.
Behavior rating scales provide a quantitative way to assess behavior. While there is still subjectivity to these tools, the thought is that data through a structured and validated tool can help us distinguish how aberrant behaviors are from the norm.
There are many excellent validated behavior rating scales for ADHD in children. The one most widely used by general pediatricians is the NICHQ Vanderbilt Assessment Scales (often referred to as "the Vanderbilt") because it is freely available (the first edition is in the public domain), easy to score, and well-validated for children 6-12 years of age (though it is considered acceptable to use outside that age range).
Despite its popularity, the Vanderbilt is often not fully utilized to its potential. Most clinicians focus on the number of symptoms rated 2 or 3 for the first 18 statements. The Vanderbilt was designed with a scoring system to provide a more granular assessment of the child’s progress with time. They recommend calculating mean scores for each ADHD subsegment, as well as the mean Performance score. This permits tracking the longitudinal progress of symptoms and performance at home and school in a quantifiable way, especially useful when medication treatment is started. The Vanderbilt is also an effective screening tool for other conditions that might mimic or coexist with ADHD, such as anxiety and learning disorders.
Calculating mean scores can be time-consuming, especially in a busy clinic setting. To speed this step up a bit, I created average score tables for quick reference. You can print these out and tape them in a convenient place in your office or have them easily accessible on your desktop computer. Just remember these average scores assume all statements have been completed (none left blank). Otherwise, you would divide by the number completed. I’ve also created for my practice a version of the Vanderbilt that can be completed online and automatically scored. Something worth considering if you have access to a survey tool, but keep in mind there still needs to be a workflow for transferring scores into the electronic medical record (EMR).
Integrating Vanderbilts into the EMR is a challenge and is often hindered by inefficient workflows. Some EMR programs incorporate the parent version of the Vanderbilt into the chart. Because teachers cannot access the child’s medical record, they still need to complete the form by hand. There are programs, like meHealth, that offer a comprehensive suite of tools to help a provider manage ADHD with EMR integration. At my practice, we give families and teachers the option of completing the Vanderbilt electronically via a survey tool. We still have to hand calculate the scores and transfer them to the EMR, but we’ve found families prefer this much more than completing it by pen and paper.
#2 Sensory Processing Disorder
It is not uncommon for a family to walk through my door with concerns about "sensory processing" or a sensory processing disorder (SPD). Some already have an SPD diagnosis, usually given by a pediatric occupational therapist (OT). Although SPD has been around since the 1970s when Jean Ayers, Ph.D. first described it, it is a controversial and uncertain condition. It is not included in the Diagnostic Statistical Manual (DSM 5). The American Academy of Pediatrics does not recommend the use of SPD as an independent diagnosis. One of the barriers to this is that a universal definition of SPD is lacking. Many children with sensory processing problems have other problems, such as inattention, hyperactivity, anxiety, social communication difficulties, tics, and repetitive behaviors. I like to describe SPD in the context of a Venn Diagram:
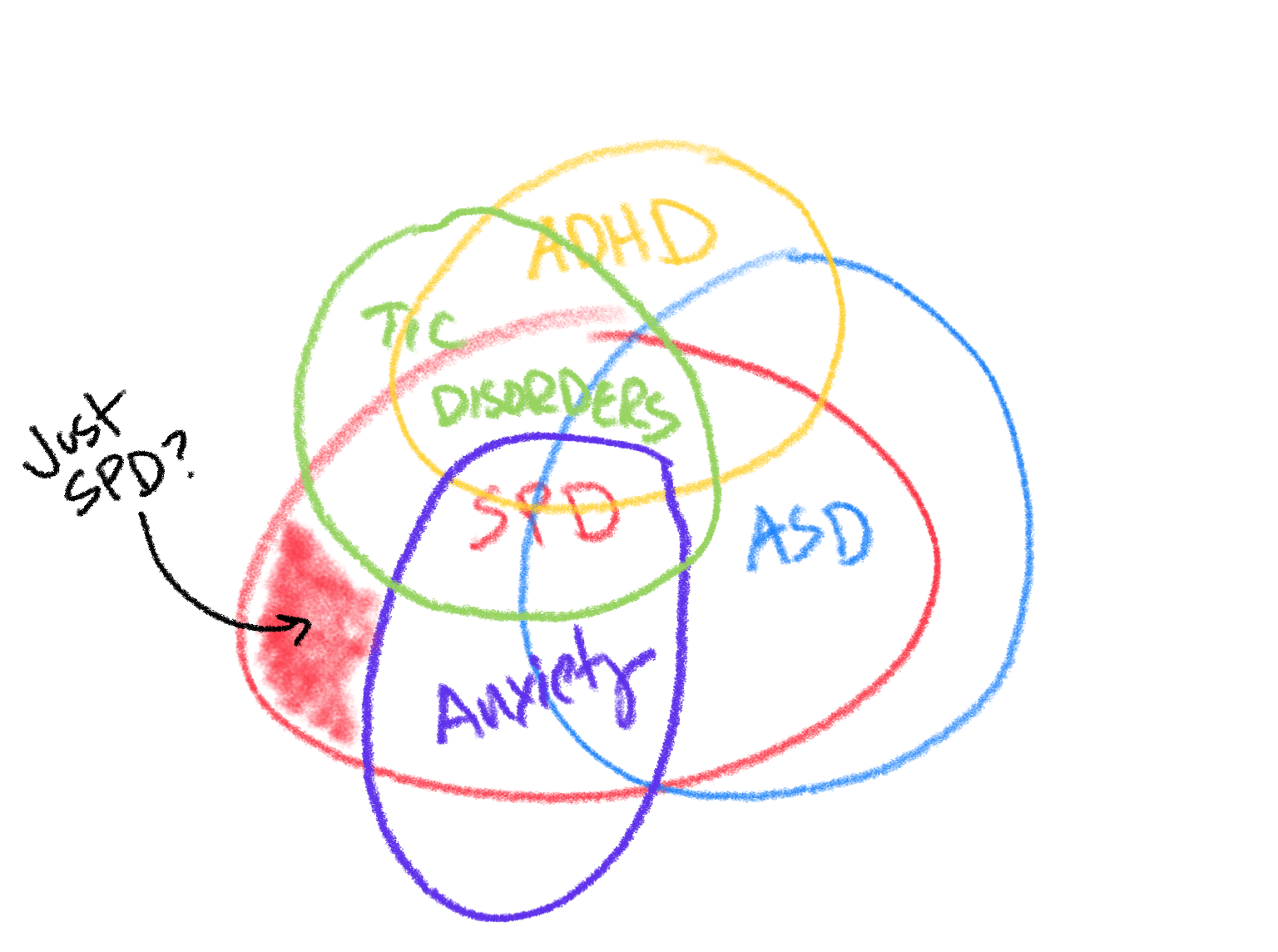
We certainly see ADHD, autism, tic disorders, and anxiety in isolation. There are clear diagnostic properties for each condition. It's not so clear with SPD. Many children with well-defined developmental disorders like autism, ADHD, and Tourette syndrome have sensory processing issues. More than a third of children with ADHD have sensory issues. Sensory differences are part of the DSM 5 criteria for diagnosing autism spectrum disorder (B-4). Not surprisingly, many children with SPD have high levels of anxiety. The bottom line is that it is tough to tease out what is what in children with sensory processing issues. Not surprising that a clinical consensus for diagnosing SPD is lacking.
DSM diagnosis or not, I am firmly in the camp that sensory processing differences exist in children (how they evolve and manifest over childhood into adulthood is another story) even though I am skeptical about SPD as a standalone diagnosis. You should always consider other disorders or conditions in any child who comes into your office with the chief complaint of “sensory processing” or "sensory issues" That being said, scientists are making serious efforts to further our understanding of sensory processing in children. There appear to be brain structural and genetic differences in children with SPD from data published in the last ten years. An important take-home point from this research is that these studies are comparing groups, not individuals. Much more work is needed before we have accurate and reliable tools to diagnose SPD in the clinical setting.
I also hesitate to make an SPD diagnosis because there is a lack of evidence-based therapies that improve children's adaptive behavior or functioning with sensory issues. Sensory-based treatments (sometimes known as “diets”) and other proposed therapeutic interventions may work from an anecdotal standpoint. Still, available research with sound methodology (i.e., randomized clinical trials) has not shown that to be the case. It is one thing for children to respond positively in a sensory gym or video game, but another if there are little or no long-term improvements in how they learn and function at school, home, team sports, scouts, birthday parties, etc. Providers must help parents think about clear and functional outcomes when pursuing these treatments that lack a lot of supporting "real world" data.
#3 ABA
I get many questions from families and providers about Applied Behavioral Analysis (ABA). It is a black box to many as an intervention for Autism. ABA is the gold standard treatment modality for children with autism and is generally recommended for young children (under the age of 5) and children with severe symptoms. It uses behavioral principles to systematically improve socially positive behaviors and decrease behaviors that interfere with learning or functioning. If you've taken an introductory college course in psychology, you'll find the concept behind ABA very familiar. ABA methods can be used in different settings: classrooms, daycares, groups, one-on-one, public places, and homes. It is an evidence-based treatment modality for autism spectrum disorders and has been shown to improve cognitive, language, and adaptive outcomes. There are many off-shoots of ABA today, such as Pivotal Response Therapy and the Early Start Denver Model. Not every child with ASD needs ABA. It would be too regimented for those with mild symptoms and relatively good adaptive and cognitive skills (e.g., Children who perhaps would have been diagnosed with Asperger syndrome in the past).
Most insurance companies cover ABA as a medically indicated treatment for children with a diagnosis of autism. Even though ABA was not designed specifically for autism, it is now almost impossible to get it covered for a child with just an intellectual disability or ADHD (an unfortunate and unintended consequence of the strong advocacy efforts by the autism community). Many PCPs contact us saying that they have difficulty getting their patients ABA. It is such a confusing process with parents often serving as the case manager for their children. These days it is not uncommon for insurance companies to require a diagnostic report by a psychologist or developmental pediatrician with specific wording and assessment tools used. There is some variation state by state. In our practice, we usually provide families with a referral to go with the diagnostic report. Families have to do their part and initiate contact with their health insurance company to start the process of identifying ABA providers in their network. These days the problem is not so much insurance covering ABA as much as it is about supply and demand with waiting times sometimes as long as four months, not made any better by the pandemic.
Many children with ASD also benefit from occupational and speech and language therapies, but not all need them. Outcomes research is mixed about these therapies. ABA, however, has the best scientific evidence in the treatment of the core symptoms of ASD and can even address problems with adaptive behaviors, such as toileting and feeding. Many other therapies could be classified as experimental or complementary/alternative (e.g., Nemechek Protocol, gluten-free diet, oxytocin, vitamin B12). Stem cell therapy is the new darling on the block, but unlike others, it has been subject to rigorous research methodology (see Duke studies) and has shown some promise, though far more subtle than hoped. I tell my families to proceed with caution when coming across a therapy that promotes a cure for autism. As the old adage goes, “If it sounds too good to be true, it probably is.”
Thanks for reading. I'll leave you a writing sample of a 6-year old child with ADHD, pre- and post- stimulant medication. It should be pretty obvious which writing sample was completed while the child was on medication.
